
Abstracts
Abstract
In this paper, we suggest that participatory research (PR) is neither a research methodology, nor uniquely associated with qualitative methods, but rather an approach to research through which stakeholders can implement quantitative, qualitative or mixed methods study designs. By illustrating three partnerships retained in our recent systematic review of PR, we highlight issues involved in partnered quantitative research. Examples demonstrate that commitment to dialogue and consensus building among partnership stakeholders is key to ensuring that methods generate scientifically valid research without creating community harm, loss of reputation, stigma or without generating feelings of denial, betrayal and exclusion.
Keywords:
- community-based participatory research,
- quantitative research methods,
- randomized controlled trials,
- quasi-experimental studies,
- negociation
Résumé
Nous suggérons que la Recherche Participative (RP) n’est pas une méthodologie et n’est pas associée uniquement à des méthodes qualitatives. La RP est plutôt une approche de recherche où les acteurs peuvent utiliser des méthodes quantitatives, qualitatives ou mixtes. Afin d’illustrer certains aspects des méthodes quantitatives en RP, nous présentons trois projets inclus dans notre revue systématique de la littérature en RP. Ces exemples montrent que s’engager dans un processus de dialogue et de consensus est crucial afin d’assurer que les méthodes de recherche employées soient valides, mais pas aux dépens des membres des communautés (par ex., stigmatisation).
Mots-clés :
- recherche communautaire participative,
- méthodes de recherche quantitative,
- essais contrôlés randomisés,
- études quasiexpérimentales,
- négociation
Article body
Introduction
Participatory research (PR) has been defined as “systematic enquiry, with the collaboration of those affected by the issue being studied, for the purpose of education and taking action or effecting social change” (Green et al., 1995). Due to the work activity involved in PR (e.g., ongoing dialogue among diverse stakeholders and interpersonal relationships), a tendency has been to understand PR as a research methodology and to conflate or confuse it with qualitative methods. We submit that PR is neither, in itself, a research methodology, nor a set of methods, but rather an approach to undertaking research. This view supports others who have stated that “although often and erroneously referred to as a research method, community-based participatory research and other participatory approaches are not methods at all but orientations to research” (Minkler and Wallerstein, 2008: 6). Other, more methodological views of PR (Jordan, 2003; Schwandt, 2007) have begun from the premise that it is intended mainly to benefit one particular group, the group from which the identified need arises; and thus the methods of creating new action-oriented knowledge should necessarily derive from that group’s epistemology. However, if we begin from the premise that PR may be the collaborative creation of knowledge by multiple groups of stakeholders, each with their disparate worldviews and means of creating, exchanging and applying knowledge, then it follows that PR is an approach to research rather than a methodology or an epistemologically-situated set of methods. In practice, members of multi-stakeholder coalitions can use the most appropriate methods for answering their research questions - including qualitative, quantitative, or mixed methods. Therefore, when researchers and non-academic stakeholders form partnerships to formulate and undertake research, the partnerships can determine how best to obtain some answers to their questions and design a study accordingly.
In this paper, our goal is to illustrate and discuss the use of quantitative methods in PR. Specifically, we highlight three partnerships from our recent realist review (Jagosh et al., 2012) that used quantitative methods to show that not only is PR an approach used in tandem with a diversity of methodological designs, but that community participation has influence over the development of methods, in a way that is not apparent in non-PR research. Our review synthesis suggests that tensions over data collection, research design and subsequent modifications to methods are more significant for academic-community partnerships that use quantitative methods including planning randomized control trials (RCTs) and quasi-experimental studies, than for partnerships that use qualitative methods solely.
Background: Clarifying PR
In this paper, we use PR as an umbrella term that includes community-based participatory research, participatory action research, action research, collaborative enquiry, and emancipatory research (Minkler and Wallerstein, 2008). With the recent understanding of the importance of applying knowledge translation to improve the uptake of research results, partners may also include policy makers and others responsible for applying research findings to effect changes (Graham et al., 2006; Parry, Salsberg and Macaulay, 2009). In addition, we define a participatory approach to mean that teams should equitably co-govern the research with co-decision making between researchers and non-academic partners occurring through all the stages of research (e.g., finalizing the research question(s), data collection, analysis and interpretation, and disseminating the findings). This does not mean that partners are necessarily involved in every decision in planning and implementation, but that there is a general consensus toward shared decision-making, co-governance and oversight throughout the research process (Shulz et al., 2005). All partnerships described in this paper meet the above criteria for PR.
Findings regarding use of quantitative methods from a recent realist review
To illustrate and discuss the use of quantitative methods in PR, we draw on examples from our recent systematic realist review of community-based participatory health research, which is described in detail elsewhere (Jagosh et al., 2012; Jagosh et al., 2011; Macaulay et al., 2011). In the realist review, we synthesized data from 23 partnerships (276 documents) to better understand the benefits of PR for research processes and health outcome goals. The partnership coalitions were comprised of academic and non-academic stakeholders, who planned, implemented, and evaluated community-based health intervention research. The duration of each of the partnerships varied, ranging from 2 to 26 years, with the longer-term partnerships planning and implementing numerous research projects in sequence over many years.
All 23 partnerships from our review employed quantitative methods in their research designs: eight used quantitative methods exclusively (observational and/or experimental designs), 11 conducted separate qualitative and quantitative research designs at different times during the partnership life course, two used mixed methods research designs exclusively, and two used quantitative, qualitative and mixed methods research designs in the various studies they conducted. An account of how each of these partnerships addressed issues relating to the co-design of quantitative methods is beyond the scope of the present report. Not all partnerships had well-documented descriptions of the challenges and facilitators to implementing quantitative methods. For these reasons, we chose three partnerships, which employequantitative methods and have also well described the process of negotiation among PR stakeholders about how these methods would be implemented in the community setting, to be used as illustrative cases.
The partnerships described here are: (a) Kahnawake Schools Diabetes Prevention Project (KSDPP), (b) The East Harlem Diabetes Center for Excellence Partnership and (c) Project BRIDGE (for HIV and substance abuse prevention in African American adolescents). The KSDPP partnership undertook multiple quantitative descriptive studies using cross-sectional and longitudinal quantitative studies: to follow the impact of school and community level healthy lifestyle interventions on elementary school children; to evaluate subgroups of children; and to evaluate the evolution of this partnership over 10 years. We will show how, through ongoing dialogue, community members and academics reached consensus in planning the evaluations to ensure respect for community values. The East Harlem and Project BRIDGE partnerships illustrate how and why established partnerships, with equitable co-governance across the stages of research, chose to conduct randomized control trials (RCTs) and quasi-experimental studies. Applying these study designs within partnerships led to debates between academic and community stakeholders concerning balancing the external validity of the research (through recruitment to a control group which does not receive the intervention) and the relationship and ethical consequences of such control group designs on the community and the academic-community relationship.
Requests were sent to key members of each of these three partnerships to confirm the accuracy of our descriptions of the work they conducted. We received responses from the Kahnawake Schools Diabetes Prevention Project and Project BRIDGE partnerships confirming that our description of the partnership was agreeable to their perspective.
Respecting community values and evaluating PR project governance and ownership
The community-academic partnership for the ongoing Kahnawake Schools Diabetes Prevention Project (KSDPP) was established in 1994 to address the community’s request that ‘something be done’ to address the high prevalence of Type 2 diabetes, and perceived increases in childhood obesity in the Kanien’kehá:ka (Mohawk) community of Kahnawake, Quebec. For this project, the community is represented through the KSDPP Community Advisory Board which has shared decision-making powers across all stages of research (Macaulay et al., 1997) and that are clearly delineated in the KSDPP Code of Research Ethics[1]. Elders of the community requested that the project focus on young children, so healthy lifestyle interventions were developed for the children attending the elementary schools, together with supporting interventions designed to reach the entire community[2].
The research began by collecting baseline data from children attending two elementary schools. The data collected from children in grades 1-6 included anthropometric measurements, questionnaires to evaluate eating, screen time and physical activity behaviors and a fitness test (Macaulay et al., 1997). Repeated measurements were taken over eight years to evaluate the impact of the interventions (Paradis et al., 2005). In addition, children in grades 4-6 also completed a 24-hour dietary recall to assess nutrient intakes: this data was also used to evaluate snacking patterns of normal weight and overweight children, with the goal of trying to better understand dietary associations with weight (Mercille, Receveur and Macaulay, 2010).
In planning these studies, the partnership followed the KSDPP Code of Research Ethics that had been developed by the researchers together with the Community Advisory Board at the outset of the project (Macaulay et al., 1997) and engaged in very detailed discussions about which data collection tools to use and how to use the results. For example, the Community Advisory Board made it very clear at the beginning of the project that the data from children attending the two elementary schools must be combined, because comparing the children attending the two schools would have been culturally inappropriate. Other discussions focused on the anthropometric measurements (height, weight and skin fold thicknesses) and who should be collecting them in order to reduce embarrassment to the children and to allay parental concerns. The final decision was that children should be measured wearing light clothing so that they felt more comfortable and the measurements were taken by a trained community nurse (as opposed to a community research assistant). When assessing snacking habits, the Community Advisory Board agreed to compare children of different weight status, provided the results should not be used to change the interventions i.e., that all the interventions remain the same for all the children and that the overweight children should not be treated differently or stigmatized. Again, researchers readily agreed to this stipulation.
In contrast to most PR ownership evaluations using qualitative methods, KSDPP also chose quantitative data collection methods to evaluate the evolution of project governance and ownership across three time-points. Questions probed into the levels of influence on various aspects of the project for each partner and culminated in the question : “Which partner is the primary owner of KSDPP at the present time?” With input from community staff, academic researchers and Community Advisory Board members a survey previously administered in the formalization (18 months) and mobilization (5 years) stages was adapted to also evaluate decisions related to the ethics of the partnership in the maintenance stage (10 years). The revised survey was administered to those involved in KSDPP during project maintenance phase (10 years). For the question “Which partner is the primary owner of KSDPP at the present time?”, linear trend analysis showed a gradual change from the Aboriginal KSDPP staff being perceived as the primary owner at 18 months, to joint staff- Community Advisory Board ownership at 5 years and to the Community Advisory Board being perceived as the primary owner at 10 years. At no time were the academic partners perceived as the primary owner. The results were useful to assess levels of governance of the project, supported the PR principle that researchers should approach Aboriginal communities with willingness to partner rather than to dictate help, and also demonstrated that long-term funding is needed to build community capacity (Cargo et al., 2011).
Planning RCTs and Quasi-Experimental Trials using a PR approach
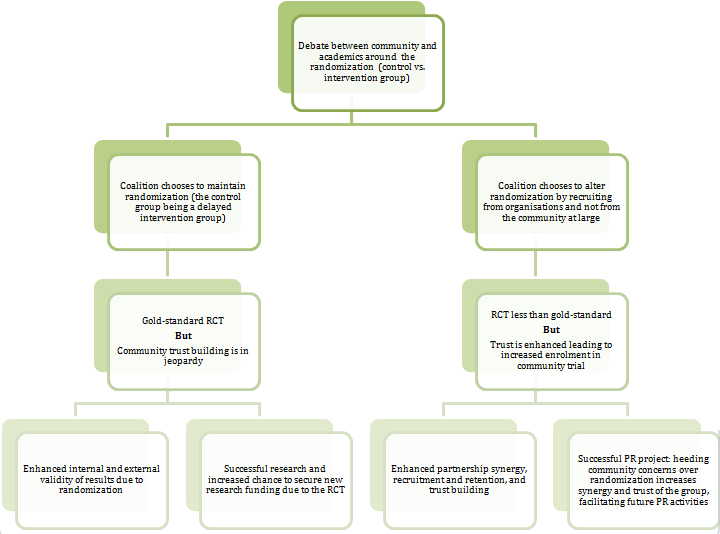
Numerous debates arose in the collaborative planning and implementation of community-based health intervention trials. These debates pertained to (a) whether or not to have a control group, (b) how to recruit participants to the intervention and control groups, and (c) how to balance external validity granted by control group design with ethics and relational considerations of having some community participants not receive the intervention. In many instances, we found that the involvement of community in planning such trials led to modifications of control group randomization to respect the interests of the community as well as the academic-community relationship. The outcome of debates between co-governing stakeholders is depicted in Figure 1.
Project BRIDGE. Project BRIDGE is a partnership which was initiated in 1997 with a mandate to plan an intervention for HIV/AIDS and substance abuse prevention. The partnership was comprised of members of a local university, an HIV prevention organization, and a church organization. The coalition was built on a relationship between one academic and one community (church) member, who had previously worked on substance abuse initiatives (Marcus et al., 2004). After three years of partnership building, conducting an extensive literature review on the study topics, and engaging in ongoing weekly meetings, the partnership applied for and received a grant to implement a three-year intervention aimed at reducing substance use and HIV/AIDS in African-American adolescents (Marcus et al., 2004). The proposed intervention included four components: (a) a cognitive-behavioural substance abuse prevention program, (b) an afro-centric prevention program based on arts, media, communication, music, and physical activity strategies, (c) an abstinence-focussed curriculum; and (d) a faith-based component (Marcus et al., 2004). To increase the external validity of the research, the academic members of the coalition proposed incorporating a comparison group which would not receive the intervention. This led to questions by the community members about how to identify the comparison group while ensuring that some adolescents not be ‘objectified’ in the process. After months of ongoing dialogue, a comparison group from a neighbouring faith-based ministry was identified and participants were given incentives for their participation. Additionally, this ministry’s staff and volunteers were offered training to fully implement Project BRIDGE in their setting at a later time.
Unlike other partnerships, the coalition decided that it was safe to maintain a randomization (control group vs. intervention group), with the understanding that the neighbouring ministry would be given the educational resources to complete their own intervention at a later date. Notably however, “Church members shifted their views about the value of comparison groups over time with the realization that the comparison group would substantiate changes they were seeing and, thus, enable the team to attract future funding and to serve larger numbers of young people” (Marcus et al., 2004: 353). Thus, no modifications to control group randomization were made.
East Harlem Diabetes Center for Excellence Partnership. The East Harlem Diabetes Center for Excellence Partnership also conducted a community trial, but the issue of control group design resulted in a different outcome. This ongoing partnership was initiated in 1997 between academics and community-based health professionals, health educators, community members, and health service and policy leaders. After lengthy initial negotiations to solidify the research agenda, the coalition agreed to focus their efforts on community-based diabetes awareness and prevention. Between 1997 and 2006 the coalition conducted a number of research activities, including a series of community events to raise awareness for diabetes prevention as well as two community-based needs assessment surveys. This work culminated in the development of a community-based RCT, which was implemented in 2007 to test the efficacy of a peer-led weight reduction program for African-American adults (Project HEED) (Goldfinger et al., 2008; Horowitz et al., 2009). At that point, the coalition guiding the RCT was comprised of “33 leaders of community-based health and social service organizations, religious institutions, and seniors’ and tenants’ organizations, as well as local activists” (Horowitz et al., 2004: 371). Among issues discussed was the fact that the coalition had to negotiate differing views on control group randomization. The community advisory board members, who were connected to community organizations, offered to recruit participants for project HEED from those organizations. However, the academics’ perspective was that such an approach to recruitment would not fulfill the requirements of random assignment and would create a biased sample. In other words, the results of the research would only be generalizable to the community participants connected to these organizations, rather than the community at large. Alternatively, community members were concerned about the narrow parameters for inclusion in the randomized trial, which would exclude many community members, resulting in local cynicism and mistrust of the program and damaging potential to disseminate and sustain the program in the future. After 10 years of successful partnering, many coalition members had an appreciation of different perspectives from past collaborative experiences. This previous co-decision making contributed to the development of trust and social cohesion which formed part of the context of the debates about random assignment. Through the lengthy negotiation process, all parties came to an agreement. The academic members agreed that random assignment could damage partnership relationships and create negative community perceptions concerning the project, which would be more costly to the project than the negative impact of quasi-random assignment to the research design. In demonstrating flexibility in the way participants would be recruited to the study, academic members led the community to feeling respected and enthusiastic about their involvement in the study: “researchers were pleased to adopt community leaders’ recommendations as these leaders moved from being reluctant to recommend potential participants to enthusiastically offering to recruit participants” (Horowitz et al., 2004: 371). Although the partnership chose to recruit participants connected to the community agency partners (vs. random recruitment from the community at large), the limitations this incurred were offset by the gains achieved through heeding community concerns. As a result, community members became more enthusiastic about the project and, with this enhanced trust and respect among stakeholders, were energized to recruit participants, thus leading to high enrolment.
Figure 1
Two pathways in the co-design of quantitative research
Discussion
This paper illustrates the use of quantitative methods by PR partnerships for planning, implementing, and evaluating health interventions, and also, for assessing partnership processes. The cases we present here exemplify how, with ongoing honest dialogue, it is possible to conduct quantitative methods and maintain respect for community concerns (Buchanan, Miller and Wallerstein, 2007). Similar to qualitative methods, designing and implementing quantitative methods at the community level requires an ongoing and very detailed dialogue between stakeholders. This is especially true if the partnerships are not well-established and if they lack the foundation of mutual trust and respect. The examples presented in this paper illustrate how years of partnership building and the cultivations of synergistic relationships can generate trust, respect, and community capacity to promote long-term partnerships and carry out sensitive quantitative study designs (e.g., baseline measurements, longitudinal studies and randomized and non-randomized trials) that would have been difficult to implement without such partnership building. Similar to qualitative methods, collaboratively designing and implementing quantitative methods requires co-learning – such that all parties express, and come to understand, all the advantages and disadvantages in making decisions on various research protocol designs. The dialogue process may require negotiations around controversial decisions, the outcomes of which depend to a large extent on how much trust and synergy has been achieved in the partnership at that point in time.
Coalition members need to ensure that such methods generate scientifically valid research without creating community harm, loss of reputation, promotion of stigma and embarrassment or without generating feelings of denial, betrayal or exclusion. At the same time, community members are well positioned to reflect how the rigour and quality of scientific methods can lead to a high quality research product which in turn increases the chances for securing future funding for research and program activities. These considerations also require ongoing, sensitive dialogue to weigh the advantages and disadvantages of various outcomes in decision-making. For some coalitions, the reality that RCTs can bring new resources into the community, for instance, may offset concerns about the negative impact of control group assignment on the community. For other coalitions, the opposite is true. In all instances, we suggest that the variables of context will determine the outcome (e.g., the degree of trust already established in the academic-community relationship, the perceived potential for harm in conducting an RCT, etc.).
The learning curve also pertains to the academic members of these partnerships who are positioned to improve their skills in communicating about quantitative methods and becoming more informed about the impact of such methods on community relations. While community members learn concepts of research design, measures and statistical analysis, it has been noted that “the academic partners require substantial mentoring from the community council […] on approaches to communicate effectively with community partners and permit respectful engagement in methods discussions” (Wells et al., 2006: S1-9). As demonstrated in the East Harlem example, community members had to explain to the academic members that the randomization of control/intervention groups would alienate members of the community, and if the message circulated within the community that the study was going to choose some people at the expense of others, overall recruitment could potentially be jeopardized. In this case, the disagreement over study design became an opportunity for academic members to learn about how the community functions, and to demonstrate humility and flexibility, which then led to renewed enthusiasm among key community stakeholders responsible for recruiting people to the intervention.
Conclusion
PR is an approach to research that can involve a variety of methodologies and methods in planning, implementing and evaluating health interventions, and also evaluating partnerships. Unlike non-participatory approaches, PR can enhance the implementation of quantitative methods at the community level by ensuring that community interests are met at every step in the process. The partnered approach also provides the opportunity for community members to learn and recognize the benefits of conducting scientific research, while at the same time protecting community interests and the academic-community relationship. The outcome of ongoing dialogue between stakeholders on quantitative research methods can vary; however, coming to consensus, regardless of the outcome, through dedicated communication, patience, understanding, humility, and flexibility strengthens the trust bond in these partnerships, which facilitates future work along a chain of project and infrastructure developments. We hope that highlighting the complex issues involved in partnered quantitative research can serve those who are embarking on such studies which involve multi-stakeholder co-governance of quantitative research designs.
Appendices
Biographical notes
Ann C Macaulay CM MD FCFP is Professor of Family Medicine at McGill University and Director of Participatory Research at McGill www.pram.mcgill.ca which is dedicated to promoting academic scholarship and capacity building. She has 25 years of experience of partnering with community members, health professionals, organisations and policy makers. She also promotes the ethics of partnered research and the need to consider the rights of the collective in addition to rights of the individual. Publication : A.C. Macaulay, L. Commanda, W. Freeman, et al (1999). Participatory research maximizes community and lay involvement. British Medical Journal, vol. 319, no. 7212. pp. 744-778.
Justin Jagosh, MA, Ph.D is a CIHR Post-Doctoral Fellow at the Department of Family Medicine, McGill University. He is a lead author on a systematic realist review assessing the outcomes of participatory research and a related study to develop key principles of integrated knowledge translation. He sits on an international dephi-panel to develop quality standards for realist and meta-narrative reviews (RAMSES Project). Publication : J. Jagosh, A.C. Macaulay, P. Pluye, et al. (2012). « Uncovering the Benefits of Participatory Research: Implications of a Realist Review for Health Research and Practice ». Milbank Quarterly, vol. 90, no. 2, 311-346.
Pierre Pluye, MD, PhD, is FRQS Research Fellow and Associate Professor, Department of Family Medicine, McGill University, Montreal, Canada. He has expertise in mixed methods studies and mixed studies reviews, and developed the Mixed Methods Appraisal Tool (http://mixedmethodsappraisaltoolpublic.pbworks.com). He studies participatory research with organizations, and the patient outcomes associated with the use of information derived from electronic knowledge resources. He has co-developed the Information Assessment Method that is used by more than 10,000 Canadian pharmacists and physicians (http://iam2009.pbworks.com).
Paula L. Bush, MSc, is a PhD candidate and part-time lecturer in the McGill University Department of Kinesiology and Physical Education, and a research assistant with Participatory Research at McGill. Her research interests include Health and Physical activity promotion and participatory research. Since 2008, she has been conducting participatory research with a Montreal YMCA. Partners have completed a mixed methods evaluation of the YMCA teen program and are currently planning subsequent research. Publication: PL, Bush, S. Laberge, & S. Laforest. (2010). Physical Activity Promotion Among Underserved Adolescents: “Make It Fun, Easy, and Popular”. Health Promotion Practice, 11,3, 79S-87S.
Jon Salsberg MA, PhD (cand.) is Associate Director of « Participatory Research at McGill » With a background in anthropology and health promotion focused on community and academic participatory research and knowledge translation, he has undertaken partnered research involving patients, health practitioners, community members, organisations, policy makers and health managers. He teaches advanced participatory research in health, in McGill University Faculty of Medicine. Publication : J. Salsberg, A.C. Macaulay (2013). « Linkage and Exchange Interventions. » in, Straus, Tetroe and Graham (Eds.). Knowledge Translation in Health Care: Moving from Evidence to Practice, 2nd Edition. Oxford: Wiley-Blackwell.
Notes
- [1]
-
[2]
See www.ksdpp.org for more details and publications.
Bibliography
- Buchanan, D. R., Miller, F. G. et N. Wallerstein (2007). « Ethical issues in community-based participatory research: balancing rigorous research with community participation in community intervention studies », Progress in Community Health Partnerships: Research, Education, and Action, vol. 1, no 2, 153-60.
- Cargo, M. D., Delormier, T., Lévesque, L., McComber, A. M. et A. C. Macaulay (2011). « Community capacity as an “inside job”: evolution of perceived ownership within a university-aboriginal community partnership », American Journal of Health Promotion, vol. 26, no 2, 96-100.
- Goldfinger, J. Z., Arniella, G., Wylie-Rosett, J. et C. R. Horowitz (2008). « Project HEAL: peer education leads to weight loss in Harlem », Journal of Health Care for the Poor and Underserved, vol. 19, no 1, 180.
- Graham, I. D., Logan, J., Harrison, M. B., Straus, S. E., Tetroe, J., Caswell, W. et N. Robinson (2006). « Lost in Translation: Time for a Map? », The Journal of Continuing Education in the Health Professions, vol. 26, no 1, 13-24.
- Green, L., George, M., Daniel, M., Frankish, C., Herbert, C. P., Bowie, W. et M. O’Neill (1995). « Review and Recommendations for the Development of Participatory Research in Health Promotion in Canada », Ottawa, The Royal Society of Canada.
- Horowitz, C. R., Arniella, A., James, S. et N. A. Bickell (2004). « Using community-based participatory research to reduce health disparities in East and Central Harlem », Mt Sinai J Med, vol. 71, no 6, 368-74.
- Horowitz, C. R., Brenner, B. L., Lachapelle, S., Amara, D. A. et G. Arniella (2009). « Effective recruitment of minority populations through community-led strategies », American Journal of Preventive Medicine, vol. 37, no 6, S195-S200.
- Jagosh, J., Macaulay, A. C., Pluye, P., Salsberg, J., Bush, P. L., Henderson, J., Sirett, E., Wong, G., Cargo, M., Herbert, C. P., Seifer, S. D., Green, L. W. et T. Greenhalgh (2012). « Uncovering the Benefits of Participatory Research: Implications of a Realist Review for Health Research and Practice », The Milbank Quarterly, vol. 90, no 2, 311-346.
- Jagosh, J., Pluye, P., Macaulay, A. C., Salsberg, J., Henderson, J., Sirett, E., Bush, P. L., Seller, R., Wong, G., Greenhalgh, T., Cargo, M., Herbert, C. P., Seifer, S. et L. W. Green (2011). « Assessing the outcomes of participatory research : protocol for identifying, selecting, appraising and synthesizing the literature for realist review », Implementation Science, vol. 6, no 1, 24, 1-8.
- Jordan, S. (2003). « Who stole my methodology? Co-opting PAR », Globalisation, Societies and Education, vol. 1, no 2, 185-200.
- Macaulay, A. C., Jagosh, J., Seller, R., Henderson, J., Cargo, M., Greenhalgh, T., Wong, G. Salsberg, J. Green, L. W., Herbert, C. P. et P. Pluye (2011). « Assessing the benefits of participatory research: a rationale for a realist review », Global Health Promotion, vol. 18, no 2, 45-48.
- Macaulay, A. C., Paradis, G., Potvin, L., Cross, E. J., Saad-Haddad, C., McComber, A., Desrosiers, S., Kirby, R., Montour, L. T., Lamping, D. L., Leduc, N. et M. Rivard (1997). « The Kahnawake Schools Diabetes Prevention Project: Intervention, Evaluation, and Baseline Results of a Diabetes Primary Prevention Program with a Native Community in Canada », Preventive Medicine, vol. 26, no 6, 779-90.
- Marcus, M. T., Walker, T., Swint, J. M., Smith, B. P., Brown, C., Busen, N., Edwards, T., Liehr, P., Taylor, W. C. et D. Williams (2004). « Community-based participatory research to prevent substance abuse and HIV/AIDS in African-American adolescents », Journal of Interprofessional Care, vol.18, no 4, 347-359.
- Mercille, G., Receveur, O. et A. C. Macaulay (2010). « Are snacking patterns associated with risk of overweight among Kahnawake schoolchildren? », Public Health Nutrition, vol. 13, no 2, 163-71.
- Minkler, M. et N. Wallerstein (2008). « Community-based participatory research for health: from process to outcomes », San Francisco, Jossey-Bass.
- Paradis, G., Levesque, L., Macaulay, A. C., Cargo, M., McComber, A., Kirby, R., Receveur, O., Kishchuk, N. et L. Potvin (2005). « Impact of a Diabetes Prevention Program on Body Size, Physical Activity, and Diet Among Kanien’keha:ka (Mohawk) Children 6 to 11 Years Old: 8-Year Results From the Kahnawake Schools Diabetes Prevention Project », Pediatrics, vol. 115, no 2, 333-39.
- Parry, D., Salsberg, J. et A. C. Macaulay (2009). « Guide to Researcher and Knowledge-User Collaboration in Health Research ». En ligne: http://www.cihr-irsc.gc.ca/e/44954.html, page consultée le 15 mai 2012.
- Schulz, A., Zenk, S. N., Kannan, S., Israel, B.A., Koch, M.A. et C.A. Stokes (2005). « CBPR Approach to Survey Design and Implementation: The Healthy Environments Partnershp Survey », dans Satcher, D., Israel, B. A., Eng, E., Schulz A. J. et E. A. Parker (sous la direction de), Methods in Community-Based Participatory Research for Health, San Francisco, Jossey Bass, 107-127.
- Schwandt, T. A. (2007). « The SAGE dictionary of qualitative inquiry », Los Angeles, Sage Publications.
- Wells, K. B., Staunton, A., Norris, K. C., Bluthenthal, R., Chung, B. W., Gelberg, L., Jones, L., Kataoka, S., Koegel, P., Miranda, J., Mangione, C. M., Patel, K., Rodriguez, M., Shapiro, M., Wong, M. et C. Council (2006). « Building an academic-community partnered network for clinical services research: The Community Health Improvement Collaborative (CHIC) », Ethnicity & Disease, vol. 16, no 1, 3-17.
List of figures
Figure 1
Two pathways in the co-design of quantitative research