
Abstracts
Abstract
Physical pain, far from being a monolithic sensation, is a complex and varied somatic response to trauma or pathophysiology. The body registers pain in response to a threat to bodily wholeness; the patient or clinician interprets pain, seeking to associate the pain with its cause (diagnosis or etiology) in order to undertake a remedy and to predict its future course (prognosis). In nursing clinical practice, where symptom assessment and management are central to the scope of practice, reading pain as sign (the clinician’s empirical observation) or as symptom (an experience reported by the patient) entails complex interpretation and translation of the body’s manifestations. This article will make explicit the semiotic dimensions of nursing pain research (and its concomitant implications for clinical practice) in two cases : Xiaomei Cong’s research into procedural pain in infants in neonatal intensive care units (NICU) and Deborah Dillon McDonald’s research into pain communication between older adults with osteoarthritis or post-surgical pain and their healthcare providers.
Keywords:
- Physical Pain,
- Symptom,
- Sign,
- Semiotics of Nursing Pain
Résumé
Loin d’être une sensation monolithique, la douleur physique est une réponse somatique complexe et variée à un trauma ou une pathophysiologie. Le corps enregistre la douleur en réponse à une menace à son intégrité; le patient ou le clinicien interprète la douleur, et cherche à associer la douleur à sa cause (diagnostic ou étiologie) afin d’établir un traitement et prédire son évolution (pronostic). Dans la pratique clinique des soins infirmiers, pratique centrée sur l’évaluation et l’encadrement des symptômes, la lecture de la douleur en tant que signe (l’observation empirique du clinicien) ou en tant que symptôme (l’expérience rapportée par le patient) implique une interprétation et une traduction complexes de manifestations corporelles. Cet article explicitera les dimensions sémiotiques des recherches sur la douleur dans un contexte infirmier (et des implications associées à la pratique clinique) dans deux cas : les études de Xiaomei Cong sur la douleur interventionnelle chez les nourrissons dans des services de soins intensifs néonataux, et les études de Deborah Dillon McDonald sur la communication de la douleur entre soignants et adultes âgés souffrant d’arthrose ou de douleur post-opératoire.
Mots-clés :
- Douleur physique,
- symptôme,
- signe,
- traitement de la douleur
Article body
Introduction
Being animate (that is, in the ancient Classical view, a besouled body or an embodied soul [Lat. anima : soul]) entails sensation, and often sentience is experienced as pain. As a biosemiotic phenomenon, pain involves a complex web of semiosis from the electrochemical to the cellular to the organic, and, in humans, to the social and cultural. For humans, pain is the occasion to make meaning (moving from sign and index to symbol), including theodicies and etiological myths to explain its existence, ethical discourses to circumscribe it, and healing discourses and practices to attribute its causes and remedy it.
Physical pain, far from being a monolithic sensation, however, is a complex and varied somatic response to trauma or pathophysiology. The body registers pain in response to a threat to bodily wholeness; the patient or clinician interprets pain, seeking to associate the pain with its cause (diagnosis or etiology) in order to undertake a remedy and to predict its future course (prognosis) (Crookshank 1923, 1989). In nursing clinical practice, where symptom assessment and management are central to the scope of practice, reading pain as sign (the clinician’s empirical observation) or as symptom (an experience reported by the patient) entails complex interpretation and translation of the body’s manifestations. As a result, nursing research into pain and pain management implicitly entails forms of semiotic analysis and use of semiosic resources in translation. This article makes explicit the semiotic dimensions of nursing pain research (and its concomitant implications for clinical practice) in two cases : Xiaomei Cong’s research into procedural pain in infants in a neonatal intensive care unit (NICU) and Deborah Dillon McDonald’s research into pain communication between older adults with chronic osteoarthritis (OA) or post-surgical pain and their healthcare providers. I have selected Cong and McDonald as exemplary cases because they are both dealing with a common phenomenon, namely pain (albeit one that is acute and procedural in infants while the other is chronic and pathophysiological in adults). Both Cong and McDonald are quantitative experimental researchers who assess the efficacy of their interventions among randomized patients. Both researchers are engaged in an analysis of patients’ signs, which the researchers translate and encode in the quantitative schemata that become their data.
The body’s semiosic resources and the nurse researcher’s or clinician’s entail transmission and translation across the biosemiotic web, the semiosphere, and they exhibit paradoxes, particularly in the presence of semiosic surplus, a profusion of signals. First, I will observe that the humanities literature about pain frequently employs the classical rhetorical topos of inexpressibility (Curtius 1953 : 159-162), while the healthcare professions are inclined to quantify and taxonomize it. Elaine Scarry (1985) placed the difficulty in expressing pain at the center of her argument, while examining the nature of material and verbal expression. Subsequently, by examining pain as a cultural phenomenon, humanities scholar David Morris (1991) aimed to counteract the inexpressibility topos and the tendency of modern Western medicine to empty pain of meaning by reducing pain to a neurological phenomenon (restoring the symbolic to a reductionistic index). More recently, physician David Biro (2010) has characterized pain as a private experience, albeit with a public side requiring metaphor and world making.
Second, I will note that according to neuromatrix theory of pain used by Cong, chronic pain does not inure patients to the sensations but further sensitizes the patients to the sensations; unlike some other signals, pain does not tend to become background noise. Third, and perhaps counter-intuitively, the acquisition of language does not unequivocally facilitate human pain communication. While Cong’s research with neonates (newborn infants) suggests that the semiosic (or at least semantic) poverty of her patients requires the nurse researcher or clinician to infer what is mediated based on an interpretation of bio-behavioral signs (which are then encoded into clinicians’ scales), McDonald’s older adult patients’ semiosic resource surplus paradoxically often constrains them because of the social scripts of the patient/clinician conversation about symptoms. Although the infant cannot describe symptoms, so the nurse must read signs, older adults’ communication about their symptoms is affected by the healthcare professionals’ questions and interruptions. In both cases, however, the nurse researcher’s analysis of clinical data requires the researcher’s assigning codes to patients’ manifestations (translating infants’ behavior or older adults’ discourse), adding other threads to the semiosic web. Indeed, there are both unidimensional and multidimensional pain assessment tools, with varying degrees of complexity in administration and varying degrees of reliability, some verbal, some visual. For example, the Visual Analogue Scale (VAS), “Can cause patient confusion,” and with the McGill Pain Questionnaire “Some patients [may be] confused by vocabulary” (National Pharmaceutical Council 2001 : 28). As Kull, Emmeche, and Favareau (2008) note, all science, indeed all knowledge, is mediated through signs, and nursing science and clinical practice are no exceptions.
I acknowledge that the seemingly facile distinction I make between “sign” (the external, objective, empirical observation of the researcher or clinician) and “symptom” (the internal, subjective report of the patient) is problematic. “Symptom,” Sebeok wryly noted :
... always appears in conjunction with sign, but the precise nature of the vinculum is far from obvious ... The relationship of sign to symptom involves either coordination or subordination... Note that only a single observer – to wit, oneself – can relate symptomatic phenomena or events, whereas an indefinite number of observers – including oneself – can observe signs.
2001 : 45-46
While the “sign” and “symptom” distinction is an apparently American health-profession usage, Thure von Uexküll (1986) prefers the German usage “subjective symptom” and “objective symptom” since, in either case, symptoms are, from a semiotic perspective, signs.
The ethical dimensions of pain deserve some amplification, particularly since, as Hoffmeyer (1993, 1996) suggests, a human ethics derived from empathy is linked to our semiosic resources, the ability to construct a self and to imaginatively place oneself in another self. The health professional’s effort to alleviate pain obviously derives from an ethical imperative to relieve suffering. However, this humanitarian motive may give the impression that pain is simply a matter of sensation in which the clinician aims to replace discomfort with comfort. In fact, as both Cong and McDonald note in their reviews of the literature, pain has less apparent, more harmful and more enduring sequelae : increased blood pressure, increased heart rate, increased production of the stress hormone cortisol (which in the short term mobilizes the body but in the long term has harmful consequences), and neurological damage, among others. Further, in older adults, as McDonald’s review of the literature shows, chronic osteoarthritis pain affects mobility, general fitness, and mood. For this reason, the American Pain Society since 1996 has defined pain as “the fifth vital sign” (National Pharmaceutical Council 2001). So the management of pain for the nurse researcher or clinician extends beyond the alleviation of suffering to the prevention of more pernicious pathologies. It should be noted, however, that some controversy attends this “fifth vital sign” characterization. The elevation of pain to the canonical status of a “vital sign” (conventionally limited to body temperature, pulse rate, respiration rate, and blood pressure) belies the discrepancy between the patient’s symptom (subjective reporting on a pain scale, for example, or a report of mobility limited by pain) and the empirically observable externally sign measured by the clinician (using a thermometer or a watch or a blood pressure gauge). The American Medical Association (AMA) has discontinued this characterization (Anson 2016), and this characterization has also been disavowed by the Joint Commission (2016). Behind this reassessment lurks the anxiety that the institution of a “fifth vital sign” (despite its semiotic ambiguity) has promoted the over-prescribing of opioid analgesics.
A Semiotic Theory of Pain?
In her studies of neonates’ pain, Cong has employed Ronald Melzack’s (2001) neuromatrix theory of pain, which bears intriguing correspondences to von Uexküll, Geigges, and Herrmann’s (1993) exposition of endosemiosis. According to Melzack, the gate control theory of pain that has dominated neurological research and practice since the 1960s, in which a fairly direct line of neurotransmission from the site of trauma or pathology to the brain, now reveals explanatory gaps. Instead, the neuromatrix theory of pain posits the creation and maintenance of a body-self neuromatrix, the creation of a “neurosignature” by means of cyclical processing and synthesis, a sentient neural hub that transduces or converts (and, I am tempted to add, “translates”) the flow of neurosignatures and of awareness, and activation of the action neuromatrix to organize patterns of movements (Melzack 2001). As Lorimer Moseley (2003) observes, pain is what the brain produces when it perceives a danger to body tissue that requires protective action, but “the notion that pain is a reliable informant of what is actually happening in the tissues is no longer tenable” (Moseley 2003 : 130). Moseley characterizes the neuromatrix and its neurosignatures as a “virtual body,” an image or representation of the embodied self combining disparate sensory data, a combination of several “representations” including the special representation of the internal and external environment and the dorsal insular cortex’s “representation of the physiological condition of the entire body” (Moseley 2003 : 132). This seems to me analogous to the notion of endosemiosis proposed by Sebeok (1976) and by von Uexküll, Geigges and Herrmann. Our body’s sentience arises in part from our cognitive signifier of the body. The body’s legibility produces a text whose signs are continuously under revision.
Others have focused their attention on a semiotic analysis of pain. For example, Ouedraogo et al. (2007) conducted an epidemological and semiotic study of sciatic pain among Black African patients (in an effort to determine if there were racial determinants of the experience of pain, finding none as it happens). Oswald (2016) employed semiotic ethnography of pain patients as consumers, examining non-verbal discourses in an effort to overcome pain’s indeterminacy and inexpressibility. Employing Heidegger and Peirce (particularly Peirce’s triadic concept of sign as object-representamen-interpretant) Kugelmann (2003) examined pain as both the bearer of meaning and a way of interpreting one’s condition. Finally, the semiotic implications of chronic pain have been well established. Priel, Rabinowitz, and Pels (1991) assert that chronic pain ceases to be an index or icon, acquiring instead a symbolic structure that requires a psychodynamic relationship between patient and clinician (rather than just a diagnostic prescriber relationship). And Quintner, Buchanan, Cohen, and Taylor (2003) describe the signified/signifier gap in the instance of fibromyalgia, a semiotic failure despite clinicians’ attempt to use its pain as an index of an empirical phenomenon.
The Challenge of Semiotic Poverty : Procedural Pain in Neonates
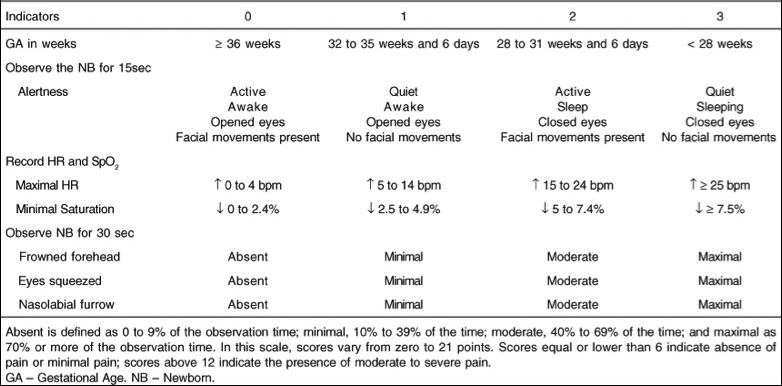
In the case of Cong’s nursing research with procedural pain in neonates (newborns), an intuitive intervention called “kangaroo care” (skin-to-skin contact with the infant placed on the mother’s or father’s bare chest) has been shown to be effective in moderating the bio-behavioral signs understood to signal pain (heart rate variability, salivary cortisol). Sometimes that pain is the side effect of life saving nursing procedures in the neonatal intensive care unit (NICU). In order to monitor the health of infants in NICUs, blood samples must be drawn regularly, using a heel stick method (puncturing the less sensitive skin of the infant’s heel) that produces procedural pain. As a safer alternative to analgesic medication, skin-to-skin care endows both bio-behavioral and psychosocial benefits on infant and parent. Its mechanism is incompletely understood but is hypothesized to include the infants’ recognition of their parents’ odor, as well as the calming effect of auditory and proprioceptive signals, like the parents’ respiration and heartbeats, each of which is a sign to which the infant responds. Of course, before and after the skin-to-skin care intervention infants cannot describe their pain to Cong, so she relies on biological signs produced through the agency of the autonomic nervous system, like heart rate variability (measured at high frequency for the parasympathetic nervous system and at low frequency for the sympathetic nervous system), oxygen saturation, and the stress hormone cortisol present in infants’ blood and saliva. In addition, there are signs produced by behavioral states; Cong “reads” infants’ faces and behavior as a text with a set of taxonomic hermeneutic keys : the Anderson Behavioral State Scoring System (ABSS) and the Premature Infant Pain Profile (PIPP). (See Figure 1 and Table 1.) The ABSS uses a numerical range scale from 1 to 12 :
1 = regular, quiet sleep; 2 = irregular sleep; 3 = active sleep; 4 = very active sleep; 5 = drowsy; 6 = alert inactive; 7 = quiet awake; 8 = active awake; 9 = very awake; 10 = fussing; 11 = crying and 12 = hard crying.
PIPP inflects behavioral alertness and facial expression with three quantitative biological signs : gestational age, heart rate variability, and oxygen saturation. A researcher like Cong or a NICU nurse must interpret the facial or behavioral state signs understood to mediate pain, translating them into a quantitative value that, through the process of clinical judgment, is then translated into clinical action.
Figure 1

Reading the Text of the Infant’s Face
Table 1
Premature Infant Pain Profile (PIPP)
Semiotic Excess : The Challenge of Chronic Pain in Older Adults
Exploring the other end of the human life span, McDonald researches pain communication with older adults, her earlier work with acute post-operative pain and her more recent work with chronic osteoarthritis pain. In this patient population one might be lulled into a sense of complacence that the adult’s access to verbal semiosic resources to describe pain’s location, quality and severity erases the clinician’s difficulty with assessing pain as with Cong’s infant patients. Paradoxically, however, the very generous semiosic resources of language, embedded as they are in cultural scripts of conversation and inflected by variables of age, gender and social role, create new difficulties. The patient and clinician may think that they have spoken and heard sufficiently, but the reality can be quite different.
As McDonald notes, there are three types of semiotic miscue. First, a clinician’s opening invitation, if phrased as “How are you today?” (or some similar phrase), employs a verbal formula that elicits a socially desirable response : “Oh, I’m fine.” This particular formula or others like it may be intended by the clinician as an invitation to disclose symptoms while it is received by the patient as merely phatic communication, which elicits a socially desirable response. Second, a clinician’s commonly used close-ended invitation, the pain scale question of “Describe your pain on a scale from one to ten,” although lacking social desirability bias, nonetheless preempts the patient’s fuller description of pain, in part by implying that the complex symptom is a clearly delineated monolithic phenomenon that can be reduced to a single signifier and to a single scale. For instance, “pain” does not adequately encompass all the kinds of discomfort that an adult patient experiences and that a clinician needs to know in order to make a health assessment. Third, the tendency of clinicians to interrupt patients typically prevents the patients from returning to their narratives or descriptions to provide more ample pain information. Finally, because the signifier “pain,” as McDonald’s research suggests, is ineffective in providing sufficient information, her research suggests that posing an open-ended question without social desirability bias and including several synonyms for “pain,” such as “Tell me about your pain, soreness or discomfort,” along with subsequent follow-up questions, is far more effective in eliciting detailed pain information. A further clinical paradox entails the common use of the pain scale question : It is not as effective in eliciting useful pain information for effective treatment, but it is required in order to justify prescribing pharmacological or non-pharmacological therapies. Thus the demands of health insurers trumps effective clinical practice for improved patient health outcomes.
McDonald’s research employs Communication Accommodation Theory (Coupland et al. 1988), which identifies five key dimensions to the social semiotic exchange between patient and clinician : attuning strategies, interpretability, discourse management, interpersonal control, and approximation. The final semiotic mediation occurs when the researcher’s data on efficacy are gathered and coded in two ways : content analysis of audio recorded patient/clinician conversations and patients’ responses post-intervention to a survey on their symptoms. Not only is pain available for semiotic analysis, but so is the discourse of patient/clinician conversation about pain.
Implications for Nursing Practice and Research
Nursing clinical practice and research across the human lifespan from infancy to older adulthood engage a variety of resources along the semiosic continuum. This article has suggested the ways in which semiotic analysis might illuminate a science and clinical field that is already fundamentally translational, in the several senses of that word. The metaphorical “translation” in modern health research and practice refers to the application of basic science into clinical practice, from lab bench to patient bedside (Rubio et al. 2010).In addition, it entails semiotic translation across symptom and sign in order to render diagnosis and treatment. Immersed in the semiosphere, the nurse researcher or clinician examines the semiosic processes of the patient’s body and appropriates the semiosic resources of human communication and meaning making, or as Pattee (2008) might characterize it, mediating the symbol-matter relationship. Applied to nursing research and clinical practice, semiotic analysis refracts clinical observations in a unique way. Nurse scholars like David Allen and Pamela Hardin (Allen & Hardin 2001; Allen 2006) have employed semiotic theory in meta-analyses of nursing theory and education, while Susan Rydahl-Hansen and Tine Rask Eriksen have used semiotic analysis to understand pain and palliative care of cancer patients (Rydahl-Hansen 2005; Rydahl-Hansen & Eriksen 2009). Finally, as Christopher Lowery and Priya Venkatesan (2008) have demonstrated, semiotic theory might also be used to enhance the accessibility of scientific communication, like that of nursing science, especially in translating nursing science to non-expert audiences.
Appendices
Biographical note
Thomas Lawrence Long is associate professor-in-residence at the University of Connecticut, School of Nursing. He has written, among others : Writing in Nursing : A Brief Guide (OUP 2017); AIDS and American Apocalypticism : The Cultural Semiotics of an Epidemic (SUNY 2005) as well as numerous book chapters and refereed articles on medicine and literature. He is currently associate editor of the journal Literature and medicine (JHU). In addition, he has curated exhibits and written works of fiction.
Bibliography
- ALLEN, D. G. (2006). “Whiteness and Differences in Nursing”. In Nursing Philosophy (7) : 65–78.
- ALLEN, D. G., & P. K. Hardin (2001). “Discourse Analysis and the Epidemiology of Meaning”. In Nursing Philosophy (2) : 163–176.
- ANSON, P. (2016). “AMA Drops Pain as Vital Sign”. Pain News Network. https://www.painnewsnetwork.org/stories/2016/6/16/ama-drops-pain-as-vital-sign
- BIRO, D. (2010). The Language of Pain : Finding Words, Compassion and Relief. New York : W.W. Norton.
- CONG, X. (2006). “Kangaroo Care for Analgesia in Preterm Infants Undergoing Heel Stick Pain”. Dissertation. Cleveland, Case Western Reserve University.
- CONG, X., S. M. Ludington-Hoe, G. McCain, & Pingfu F. (2009). “Kangaroo Care Modifies Preterm Infant Heart Rate Variability in Response to Heel Stick Pain : Pilot Study”. In Early Human Development (85)9 : 561-567.
- CONG, X., S. M. Ludington-Hoe, & S. Walsh. (2011). “Randomized Crossover Trial of Kangaroo Care to Reduce Biobehavioral Pain Responses in Preterm Infants : A Pilot Study”. In Biological Research in Nursing (13)2 : 204-216.
- COUPLAND, N., J. Coupland, H. Giles, & K. Henwood (1988). “Accommodating the Elderly : Invoking and Extending a Theory”. In Language in Society (17) : 1-41.
- CROOKSHANK, F. G. (1923, [1989]). “The Importance of a Theory of Signs and a Critique of Language in the Study of Medicine”. In C. K. Ogden & I. A Richards, The Meaning of Meaning : A Study of the Influence of Language upon Thought and of the Science of Symbolism. New York : Harcourt, Brace, Jovanovich : 337-355.
- CURTIUS, E. R. (1953). European Literature and the Latin Middle Ages. Willard R. Trask, (trans.), New York, Harper & Row : 159-162.
- HOFFMEYER, J. (1993 [1996]). Healing – On Ethics : Reuniting Two Stories in One Body-Mind. Signs of Meaning in the Universe. Barbara J. Haveland (trans.), Bloomington : Indiana University Press : 129-146.
- JOINT COMMISSION. (2016). Joint Commission Statement on Pain Management. https://www.jointcommission.org/joint_commission_statement_on_pain_management/
- KUGELMANN, Robert. (2003). “Pain as Symptom, Pain as Sign”. In Health : An Interdisciplinary Journal for the Social Study of Health, Illness and Medicine (7) : 29-50.
- KULL , K., C. Emmeche, & D. Favareau. (2008). “Biosemiotic Questions”. In Biosemiotics (1) : 41–55.
- LOWREY, C. H., & P. Venkatesan. (2008). “Making Science Accessible : A Semiotics of Scientific Communication”. In Biosemiotics (1) 253–269.
- MCDONALD, D. Dillon. (2009). “Older Adults’ Pain Descriptions”. In Pain Management Nursing (10)3 : 142-148.
- MCDONALD, D. Dillon, & J. Fedo. (2009). “Older Adults’ Pain Communication : The Effect of Interruption”. In Pain Management Nursing (10)3 : 149-153.
- MCDONALD, D. Dillon, M. Freeland, G. Thomas, & J. Moore. (2001). “Testing a Preoperative Pain Management Intervention for Elders”. In Research in Nursing & Health (24) : 402-409.
- MCDONALD, D. Dillon, M., LaPorta, & M. Meadows-Oliver. (2007).“Nurses’ Response to Pain Communication from Patients : A Post-Test Experimental Study”. In International Journal of Nursing Studies (44) : 29-35.
- MCDONALD D. Dillon, & S. L. Molony (2004). “Postoperative Pain Communication Skills for Older Adults”. In Western Journal of Nursing Research (26) : 836-852.
- MCDONALD, D. Dillon, M. Shea, J. Fedo, L. Rose, K. Bacon, K. Noble, & J. Stewart. (2008). “Older Adult Pain Communication and the Brief Pain Inventory Short For”. In Pain Management Nursing (9)4 : 154-159.
- MCDONALD, D. Dillon, M. Shea, L. Rose, & J. Fedo. (2009). “The Effect of Pain Question Phrasing on Older Adult Pain Information”. In Journal of Pain and Symptom Management (37)6 : 1050-1060.
- MCDONALD, D. Dillon, G. J. Thomas, K. E. Livingston, & J. Scott Severson. (2005). “Assisting Older Adults to Communicate Their Postoperative Pain”. In Clinical Nursing Research (14)2 : 109-126.
- MELZACK, R. (2001). “Pain and the Neuromatrix in the Brain”. In Journal of Dental Education (65)12 : 1378-1382.
- MORRIS, D. B. (1991). The Culture of Pain. Berkeley : University of California Press.
- MOSELEY, G. L. (2003). “A Pain Neuromatrix Approach to Patients with Chronic Pain”. In Manual Therapy (8)3 : 130-140.
- NATIONAL PHARMACEUTICAL COUNCIL. (2001). “Assessment of Pain”. Pain : Current Understanding of Assessment, Management, and Treatments. Reston, VA : National Pharmaceutical Council. http://americanpainsociety.org/uploads/education/section_2.pdf
- PATTEE, H. H. (2008). “Physical and Functional Conditions for Symbols, Codes, and Languages”. In Biosemiotics (1) : 147–168.
- PRIEL, B., Rabinowitz, B., & Pels, R. J. (1991). “A Semiotic Perspective on Chronic Pain : Implications for the Interaction Between Patient and Physician”. In British Journal of Medical Psychology (64) : 65–71.
- QUINTNER, J., Buchanan, D., Cohen M., & Taylor, A. (2003). “Signification and Pain : A Semiotic Reading of Fibromyalgia”. In Theoretical Medicine and Bioethics (24) : 345-54.
- RUBIO, D. McGartland, et al. (2010). “Defining Translational Research : Implications for Training”. In Academic Medicine (85) : 470-475.
- RYDAHL-HANSEN, S. (2005). “Hospitalized Patients Experienced Suffering in Life with Incurable Cancer”. In Scandinavian Journal of Caring Science (19) : 213–222.
- RYDAHL-HANSEN, S., & T. Rask Eriksen. (2009). “How are Verbal Cues and Signs of Suffering Expressed and Acknowledged Within Palliative Nursing?” In Vård i Norden/Nordic Journal of Nursing Research and Clinical Studies (29) 3 : 42-46.
- SEBEOK, T. A. (1976). Contributions to the Doctrine of Signs. Lisse : The Peter de Ridder Press.
- SEBEOK, T. A. (2001). Galen in Medical Semiotics. Global Semiotics. Bloomington : Indiana University Press : 45-46.
- SCARRY, E. (1985). The Body in Pain : The Making and Unmaking of the World. New York : Oxford University Press.
- VON UEXKÜLL, T. (1986). “Medicine and Semiotics”. In Semiotica (61)3/4 : 201-217.
- VON UEXKÜLL, T., Werner G., & Jörg M. H.. (1993). “Endosemiosis”. In Semiotica (96)1/2 : 5-51.
List of figures
Figure 1
Reading the Text of the Infant’s Face
List of tables
Table 1
Premature Infant Pain Profile (PIPP)